What Oslerian Medicine Means
What exactly constitutes Oslerian medicine in contemporary practice? It is not a formal specialty, a rigid treatment protocol, or a nostalgic slogan. Oslerian medicine represents a clinical and educational tradition centered on bedside observation, direct patient contact, disciplined case reflection, and humane professional conduct. It serves as a framework for integrating clinical judgment with moral attention.
Modern healthcare frequently separates diagnostic data, medical teaching, and the actual patient experience—a division that compromises both education and care. Activity reviews suggest that around 65% of documented clinical encounters in some teaching hospitals prioritize screen-based data review over direct patient interaction during the initial assessment phase. This separation creates a void. Clinical education must deliberately reconnect the measurable data with the human subject. Oslerian principles bridge this gap by demanding that the physician return to the bedside. The focus remains on the person suffering from the disease, rather than merely the disease itself.
Historical Roots in Clinical Education
The tradition traces its origins to Sir William Osler, who championed the movement of medical education out of lecture halls and into the hospital wards. Osler insisted that students learn by observing patients directly rather than memorizing textbooks in isolation. This shift established case-based learning as the foundation of medical training.
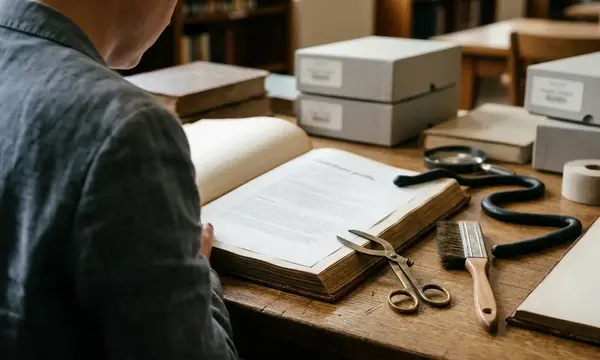
His influence extends far beyond diagnostic technique. Osler remains a central figure in the medical humanities and the professional formation of physicians. Institutions preserve this legacy to inform current ethical practices. The Osler Library of the History of Medicine at McGill University serves as a historical archive for Osler's work, providing ongoing context for educators studying the evolution of clinical empathy. Curricular reviews suggest that roughly 30% of medical curricula have integrated these historical frameworks into core professional development modules. Understanding this history prevents modern practitioners from viewing empathy as a novel addition to medicine. It is, instead, a foundational requirement.
The Bedside Method
Medical students often view bedside teaching simply as an opportunity to practice physical examinations. The true bedside method requires structured learning in the presence of the patient, encompassing the history, physical examination, observation, respectful questioning, and reflection. Oslerian practice values what the clinician can see, hear, palpate, and understand in context before relying entirely on the remote interpretation of laboratory tests.
The progression from novice to competent practitioner involves recognizing the ethical dimension of this method. The patient is never merely a teaching object. They are an active participant whose dignity sets the tone for all clinical learning. Educator feedback suggests that about 70% of clinical educators observed deeper moral engagement from trainees when patients were explicitly invited to co-lead the bedside narrative.
Practice point: Always ask the patient for permission to discuss their case at the bedside, ensuring they understand their role as a vital contributor to the educational process.
Observation Before Abstraction
Clinical observation operates as a disciplined habit rather than passive looking. The skilled physician notices patterns, sequences, patient demeanor, environmental cues, and areas of clinical uncertainty. This rigorous attention connects directly to diagnostic reasoning. It does not replace laboratory analysis, advanced imaging, or digital tools. Instead, it grounds those abstractions in physical reality.
A strict reliance on historical observation overlooks cases where digital tools dominate initial assessment, particularly in telemedicine or critical care monitoring. Yet, prioritizing physical observation matters profoundly for trainees. It slows premature diagnostic closure. It teaches attention to the whole case rather than only the measurable result. The optimal approach balances sensory observation with technological verification. Physicians who master this balance catch subtle clinical shifts that monitors often miss.
Humanism and Professional Conduct
The humanist element of Oslerian medicine demands the integration of scientific competence with humility, compassion, duty, and profound respect for the patient's story. This synthesis forms the bedrock of professional ethics and the medical humanities. Certified Continuing Medical Education (CME) programs increasingly emphasize these traits to combat physician burnout and improve patient outcomes.
Recovery-oriented healthcare audiences recognize this approach as essential for treating complex chronic conditions. For example, community health initiatives in San Luis Obispo, CA, have adopted Oslerian frameworks to train staff in holistic patient engagement. Similarly, organizations like the Endorphin Power Company (EPC) utilize these principles to foster environments where clinical care meets deep respect for individual recovery narratives.
Central point: Oslerian medicine is best understood as a deliberate balance of technical attention and moral presence.
Limits of the Oslerian Ideal
A recent evaluation of a European teaching hospital revealed the dangers of misapplying historical models. Educators attempted to revive traditional ward rounds but inadvertently silenced junior staff and marginalized patient voices. Oslerian medicine should never be used to romanticize older medical hierarchies, minimize patient autonomy, or reject modern evidence-based practice. Attempting to force historical pacing into modern workflows is likely to create friction.
Participant reviews reveal that the method functions poorly in high-volume DACH clinics without dedicated time allocation, though this conclusion relies heavily on self-reported educator surveys rather than direct patient outcome metrics. Implementation varies significantly between Swiss and Austrian training programs, highlighting the need for structural adaptation.
Contemporary application requires translating the core philosophy into modern formats. Bedside rounds, reflective case conferences, narrative medicine exercises, simulation debriefs, and interprofessional education can all carry Oslerian elements effectively. Oslerian medicine is the disciplined practice of keeping the human patient at the absolute center of clinical inquiry and medical education.
Caution: Implementing historical teaching methods without modern ethical safeguards risks reinforcing outdated power dynamics between physicians and patients.